Up until now, Canada has been without a national diabetes strategy. But thanks to the work of tireless advocates and diabetes organizations, on June 21, 2021 Bill C-237 an Act to Establish a National Diabetes Framework, was passed by the Senate.
The passage of the bill means that the federal government is poised to take on the work proposed by Liberal MP Sonia Sidhu who was the sponsor of this Private Member’s Bill C-237, National Framework For Diabetes Act.
Bill C-237 was inspired by a Diabetes 360° initiative first proposed by Diabetes Canada with support and input from JDRF Canada and other diabetes organizations. Diabetes 360° aims to develop meaningful targets designed to stem the rising tide of diabetes based on an innovative model that was used globally to tackle HIV/AIDS.
The need for a comprehensive diabetes strategy is becoming increasingly important given the rising costs of complications associated with diabetes and the rapid rise in incidence over the past decade.
The first reading of the bill took place in February, 2020 and has taken just over a year to go from proposal to assent.
Senator Nancy Hartling, who added her voice in support of Bill C-237, spoke passionately when she said,
“We don’t need to start from scratch, colleagues; there is a lot of expertise right here in Parliament, including Diabetes Canada’s Diabetes 360° framework. In addition, we already have two all-party parliamentary diabetes groups that foster dialogue, policies, best practices and awareness on diabetes.
Diabetes 360° was developed after extensive consultation with stakeholders, including experts, health care providers, governments, researchers and the diabetic community. It is based on the UN AIDS model, which combined successful 90-90-90 targeting strategy with the treatment as a prevention model to make ambitious inroads against HIV/AIDS epidemics.
Diabetes Canada saw an opportunity to adapt the strategy to diabetes and developed the 360 targets, which are composed of the four 90s: one, prevention and elimination of health inequities; two, awareness and screening; three, achievement of health outcomes through treatment and technology; and four, engaging in a patient-centred approach to reduce rates of diabetes and improve overall well-being.
The four 90s are achievable. They require a consistent, coordinated approach and the cooperation of all levels of government. Bill C-237 aims to facilitate this process and provides all the tools our government needs to do it.”
What does the bill being passed mean?
(1) That the Minister of Health must, in consultation with the representatives of the provincial governments responsible for health, Indigenous groups and with other relevant stakeholders, develop a national framework designed to support improved access to diabetes prevention and treatment to ensure better health outcomes for Canadians.
(2) The national framework must include measures to
(a) explain what diabetes and prediabetes are;
(b) identify the training, education and guidance needs of health care and other professionals related to the prevention and treatment of diabetes, including clinical practice guidelines;
(c) promote research and improve data collection on diabetes prevention and treatment;
(d) promote information and knowledge sharing in relation to diabetes prevention and treatment; and
(e) take into consideration any existing diabetes prevention and treatment frameworks, strategies and best practices, including those that focus on addressing health inequalities.
And that the Minister must hold at least one conference with the persons referred to in subsection (1) for the purpose of developing the framework.
JDRF congratulates and thank MP Sonia Sidhu, Diabetes Canada, along with the other diabetes advocates who have worked together to advocate for Diabetes 360°, a strategy and framework to advance research to treat, prevent and cure diabetes.
The passage of the Bill is testament to the power of collaboration, and we recognize Diabetes Canada for leading the charge.
We look forward to working with the government to improve the lives of Canadians living with diabetes.
There has been some great progress made recently towards greater access to diabetes devices and federal commitments to funding and incorporating a national diabetes strategy. These have only been achieved through collaboration with partners and other diabetes organizations and on the strength of our volunteers.
We rely on a network of passionate volunteer advocates to help Canada’s decision-makers understand the impact and severity of type 1 diabetes (T1D) and what needs to be done to improve the lives of those living with this disease.
We have a variety of volunteering opportunities and are always open to suggestions. Please visit our website to see some of the ways our volunteers help and consider joining us too. www.jdrf.ca/get-involved/advocate
Access for All was launched in 2019 and has already driven major change. We are fortunate to have some of the most powerful young voices in the country advocating for our mission. These dedicated individuals have rallied communities across the country, and now several provinces and territories are in the process of revisiting their coverage and considering expanded access.
Diabetes devices are not a luxury, they are lifesaving pieces of equipment that help people living with T1D more closely monitor their blood glucose levels, helping to prevent hypo and hyperglycemic episodes and hospital visits.
‘Paying out of pocket is beyond what I can afford. I don’t consider my son’s CGM an ‘optional’ medical device…I’ll do whatever I need to do, and I know I’m not alone in this,’ says Nadine, parent of a child with T1D.
JDRF is pleased to announce that two more provinces recently added coverage options for continuous glucose monitors (CGM) over the past month, a great step forward in our goal of Access For All across the country.
On May 26, 2021, the Régie de l’Assurance Maladie du Quebec or RAMQ announced that it would start providing coverage of the Dexcom G6 CGM for people living with type 1 diabetes (T1D), age two years or older.
This announcement marks a significant accomplishment in increasing access to life changing technology used in the management of T1D for people in the province, as they will now also be able to order and pick up their Dexcom CGM supplies directly through their local pharmacy.
To receive coverage for Dexcom G6 under RAMQ, an individual must meet the eligibility requirements for the Public Insurance Plan. In addition, you must be:
Living with T1D and aged 2 years or older. AND, you must have one or more of the following:
Failure to achieve an appropriate glycated hemoglobin (HbA1c) value despite taking prescribed medications and testing blood sugar regularly; or
Have experienced frequent episodes of hypoglycemia in the past year despite following a treatment plan; or
Are not able to recognize or report symptoms of hypoglycemia.
A local pharmacist can than provide a prescription for RAMQ approval, which initially lasts for six months and must be renewed every 12 months following.
In 2020, JDRF turned its attention west to British Columbia working with the community to advocate for better diabetes device coverage. This included a pre-budget submission, holding community consultations across the province, and JDRF participated alongside Diabetes Canada and Type 1 Together in public and stakeholder consultations held by BC Pharmaceutical Services in August and September.
On June 11, 2021 British Columbia announced that it will begin covering Dexcom G6 continuous glucose monitoring (CGM) for those requiring insulin therapy aged 2+ who meet eligibility criteria. This coverage is effective as of June 11, 2021. An estimated 20,000 British Columbians are expected to qualify helping them better manage their disease.
In BC, Dexcom G6 sensors and receivers will be fully covered for those whose family income is <$30K annually or who are on government assistance and mostly covered for everyone else. Eligibility criteria is fairly broad and the government expects some 20K people to qualify.
British Columbia and Quebec now join Saskatchewan, Manitoba and the Yukon in covering CGM for some or all with T1D. Quebec, Ontario, Saskatchewan and the Yukon also cover Flash GM.
JDRF is very pleased with these announcements as a step towards universal coverage of life-saving diabetes devices, but there is still work to be done for true Access For All.
It is our hope that in the future other CGM products and the Flash GM will be covered in BC and QC – and the remaining provinces as well. Diabetes is a very individual disease that affects different patients differently. We believe in choice when it comes to treatment options, and for patients in consultation with their health care providers to decide on their best course of treatment.
Summer is here and as Canadians are getting vaccinated against COVID-19, we have decided to take a break from our live Let’s Talk T1D events on Microsoft Teams, and package them in a way that is more convenient for the summer months.
More Canadians are getting vaccinated against COVID-19 and restrictions across the country are easing. The light at the end of the tunnel is getting brighter. However, we know that the past 16 months have not been easy, and we’ve all faced different challenges in our lives, including mental health challenges, especially for those impacted by type 1 diabetes (T1D). We know that this pandemic may have been a contributing factor to diabetes burnout and pandemic fatigue.
As part of this month’s Let’s Talk T1D – education series, we are bringing you information on this topic- one that important to you, as we saw in the results of a survey we sent out to the T1D community.
In this email you will find links to two videos discussing diabetes burnout and pandemic fatigue. We reached out to Dr. Michael Vallis, Registered Health Psychologist out of Dalhousie University, and Cathy and Anne Pettigrew, a mother and daughter to answer some of your questions.
In the videos they will address some common questions such as:
What is diabetes distress and burnout and how common is it for people with T1D to experience it?
What are some of the signs to watch out for that a person might be experiencing diabetes distress or burnout? (Are they emotional, physical, or both?)
Were concerns about diabetes distress and burnout intensified during the pandemic?
When is it time to seek help?
What would you like the T1D community to know about prioritizing their emotional health and well-being?
We thank Dr. Vallis and Anne and Cathy Pettigrew for providing their time, expertise and willingness to share so that we can share with our community and help other who may be experiencing the same know that they are not alone, and support is available.
Type 1 diabetes is an autoimmune disease resulting in a lifelong dependency on insulin treatment and a risk of serious long-term complications. The cause of the disease is unclear, although both genes and factors in the environment seem to be important. As new cases of this burdensome and costly disease are on the rise in almost every country around the world, finding ways to prevent and better treat type 1 diabetes are top research priorities.
In the past decade, research has shown that changes in the gut microbiome – the microbial community that colonizes the intestine – precede the onset of type 1 diabetes in young children. Most of these studies highlight a potential link in the first years of life when the microbiome is highly dynamic and heavily influenced by environmental factors such as mode of birth delivery, diet, infections, and antibiotic use. JDRF and other funders have invested heavily in this area, supporting studies such as the DIABIMMUNE Study, BABYDIET, and TEDDY, which all helped to point researchers towards new therapeutic opportunities. In addition, for many years, JDRF led an international consortium that brought researchers working in this area together on a regular basis to share ideas, compare data, and accelerate progress.
The field is now focused on testing whether manipulation of the microbiome with drugs or diet can delay or even prevent the disease altogether. Other studies are attempting to figure out how changes in the gut microbiome could signal a person is at risk of developing type 1 diabetes.
Dr. Jayne Danska, a professor at the University of Toronto Faculty of Medicine and a senior scientist at The Hospital for Sick Children, is working at the cutting edge of this field. In late 2019, she was awarded a $2 million CAD team grant from JDRF and the Canadian Institutes for Health Research (CIHR) to advance her work studying the role of the gut microbiome in altering risk and progression of type 1 diabetes. She and her team previously showed that deliberate manipulations of the gut microbiome can inhibit autoimmune responses in an experimental model of type 1 diabetes. The new five-year project seeks to understand how environmental changes influence the gut microbiome in infants with genetic risk for type 1 diabetes. The team will attempt to define exactly what risk-associated microbes do inside a developing infant, and how they affect the immune response to either protect against or potentiate the disease. The ultimate objective of Dr. Danska’s work is to identify new therapeutics to prevent type 1 diabetes.
We are facing a moment in time that can forever change the landscape of type 1 diabetes research, with better treatments and cures on the horizon. JDRF is striving to speed up research progress in any way we can. We are constantly scouting for the best ideas, the brightest talent and the innovative project that will bring us the next real breakthrough.
We’re heading into the summer, and after a long Canadian winter, many of us are more than ready to head outdoors. But the summer season also means some different planning when managing type 1 diabetes (T1D).
Please find below some tips and suggestions to help you get the most out of the sunny days.
COVID-19 Safety
Each province and territory has its own COVID-19 safety and re-start plans in place. Please check your province or territory’s health authority website for information on gathering sizes, indoors vs. outdoors, patios and other recreational amenities.
5 tips for managing T1D in the summer
Stay hydrated. Hot weather can quickly dehydrate anyone. To prevent blood-sugar spikes from dehydration, drink water throughout the day.
Test blood-sugar levels frequently. Hot temps can cause unpredictable swings in blood-sugar levels.
Protect your gear. Keep your pump covered and your insulin cool. Heat can make insulin less effective and can cause pumps to malfunction. There are cooling cases specifically for insulin that can help you manage your supply.
Pack snacks. Before any summer road trips or outings, be sure to stock up with snacks to help prevent blood-sugar lows. And try as best you can to stay on your food schedule.
Exercise in the mornings or at night and plan any outdoor exercise for the cooler parts of the day. Exercising in the heat can cause heat exhaustion and make staying in a healthy range difficult. Be aware of how much you’re sweating. Too much moisture can damage some pumps, so make sure to check it while working out.
It’s also really important to wear sunscreen. Everyone should be protecting their skin from harmful UV rays, but with T1D, the need to wear sunscreen is extra important. Sunburns are a stress on the body and can cause blood-sugar spikes. Use SPF 30 or higher.
The Science of Summer
Heat can cause both unanticipated highs and lows in blood-sugar levels. As well, dehydration is common in the summer and can lead to blood sugar spikes as the glucose gets more concentrated in the bloodstream due to decreased blood flow in the kidneys.
The heat can also cause blood-glucose lows. As the temperature rises, the body’s blood vessels dilate, speeding up insulin absorption and increasing the risk of hypoglycemia. This is especially true while exercising, as working out already increases blood flow.
It’s essential to stay hydrated and find shade or go inside for a break when you feel overheated.
Summer Travel Checklist
Summers are made for getting away! If you’re planning on a day trip, or a longer excursion to a cottage or beach house, here are some things to consider taking with you:
A travel letter from your doctor with written approval to travel with insulin and syringes (recommended)
Insulin (and syringes or pens, depending on what you use)
Test strips
Lancets
Ketone test strips
Back-up snacks
Emergency glucagon
Supplies for any diabetes devices you use, for e.g. blood glucose meters, continuous glucose monitors (CGM) Flash GMs, or insulin pumps
Pack twice as much medication and supplies as you think you’ll need (just in case!).
If you’re using an insulin pump, many manufacturers offer loaners for travel. Consider asking for one as a back-up.
If you’re flying, keep all of the above, especially your insulin, in a carry-on bag. Medications should be kept in a clear plastic bag, ready for airport security. Don’t store insulin or a CGM/Flash GM in checked luggage as the cargo holds can have extreme temperatures and could damage them before you land.
How to safely drink with T1D
T1D should not keep you from enjoying a margarita or frosty mug of beer.
Be mindful of your alcohol consumption, especially in the sun, as it can affect your body’s ability to regulate temperature. In general, stick to low-sugar options, stay hydrated (with water!) and don’t drink on an empty stomach.
Joseph Segal is a 96-year-old World War II vet and renowned business tycoon. As the founder of Fields stores and President of Kingswood Capital Corporation, Joseph Segal has built an impressive empire, but perhaps his most tremendous success comes in the form of his and his family’s philanthropy. Recently, JDRF was the recipient of his family’s incredible generosity, receiving a $1 million contribution to fund the JDRF Centre of Excellence at the University of British Columbia as part of its Campaign to Accelerate.
This Centre will be the first of its kind in Canada, among just four others worldwide. In Vancouver, world-class researchers are poised to bring therapies to the clinical testing stage to cure T1D and positively impact other autoimmune diseases.
The JDRF Centre of Excellence will be a game-changer for T1D research. Joseph and Rosalie Segal and their family have helped to set that change in motion.
JDRF had the opportunity to speak to Joseph and his grandson Danny Miller about what prompted their contribution. See the interview below from May 13, 2021:
JDRF: Mr. Segal, Please tell us more about what causes you feel strongly about and why?
Joseph Segal: I could sum it up in one word: everything.
We feel that every cause that has a genuineness to it is important. So I could say mental health, I could say Vancouver General Hospital, I could say education because education is the answer to most of the tragedy in the world. So every cause is important. But, there are other causes that most people don’t look at when you have a situation – an individual who needs a little bit of help – maybe $5,000, maybe $3,000, perhaps $10,000; and they don’t know where to turn. They have nowhere to turn. Those are causes that are below the surface, and those are the causes that are important because it gives the individual a little bit of encouragement. It makes the individual feel that you care. Those are the causes that go unseen. But those are the causes that have as much impact as giving to what everybody else gives to.
So, you have to have somebody who you can look to who will give you a hand. That’s simple. And that’s a very necessary part of society that is, to a large degree, overlooked.
JDRF: Mr. Segal, why is giving important to you personally?
Joseph Segal: You have an obligation in society to give because you truly feel you want to give. That is a different situation than giving because you have to give.
I can remember days when I didn’t have that much, and my first major contribution was $100,000, which was the value of my house. So, I was essentially giving away my house. But, I thought, I’ll make it back. So, it’s not a question of saying, I’m giving back – you have to say I’m giving what I can.
The individual who gives $2,000 is equally as important as the individual who gives $1 million because nobody gives anything that they’re going to miss. But the $2,000 contributor is probably going to feel it more than the $1 million contributors.
JDRF: Mr. Segal, how do you and Rosalie make decisions on what to fund?
Joseph Segal: Most people probably have a dialogue, and they try to determine if it’s important or not important. I’ve been married 73 years next month, and in 73 years, I have never, ever had a difference of opinion or discussion around any charity that we decided to support. She has charities that I don’t even think about to support. I have charities, make a decision, make a commitment, and fulfill the commitment. That’s the end of it. We do it together.
There has never been a difference of opinion to what is necessary because when the cause is right, it doesn’t matter who makes the decision. If you can, you support the cause to whatever degree you feel inclined.
JDRF: Mr. Segal, what made you become our first donor to the JDRF Centre of Excellence at UBC?
Joseph Segal: There are many reasons that I did it, but the first reason is that it’s worthy.
There are many causes that are universal, and diabetes is universal. It’s an important step towards solving a major problem. It is like the vaccination for COVID-19, if you didn’t have it, what would you have? Chaos around the world. So, it is not about the obligation to find a solution but about the will to find a solution to one of the problems that are so important in society. Juvenile diabetes is one thing, and then as you become an adult, you still have diabetes because there is no solution to it. Because I have had an exposure with a family member or two who have suffered from diabetes, and it’s a debilitating disease if you don’t manage it. People that don’t have it probably don’t understand the necessity of managing it properly.
So, you’re not just doing a good job, you’re fulfilling a major need for the community, and if you get this off the ground, if they find just a little bit of a cure – a partial cure – open the window and let the fresh air in, that’s what you’re trying to do.
Once you find a solution, you will enhance the lives of so many people, and that was the reason.
JDRF: Mr. Segal, a major component of the Centre of Excellence, is being flexible and adapting as the research changes. How does that adaptability align with your business ethos?
Joseph Segal: If you want to be successful in life, you need flexibility. You can go down the road, and you can say “I am on the right road” and you can drive 100 kms, and then you’ll say “I’m maybe on the wrong road”. So, when you’re into research, and I’m not familiar with research, but I can imagine that when you’re in research, you’ll find something you didn’t anticipate. And maybe that opens up a whole new road, and you pursue that road instead of the other road.
Without flexibility, it can take twice as long to find the answer and find the road.
You have to be optimistic too. You have to believe that the mission you’re on will have an end and that you’ll be happy with it. If all your researchers have the same attitude, then their profession is going to yield results.
JDRF: Mr. Segal, where did your philanthropic value system come from, and how have you instilled it throughout your family?
Joseph Segal: When we got married 73 years ago, I didn’t have anything; I was in the army and overseas in Europe (Belgium, Germany). When I came back and saw my wife, I said “That’s the girl of my dreams,” and I married her. We both set the example for our children and, fortunately, they have the same attitude. They’re involved in different areas and different communities. I attribute that entirely to my wife.
I don’t have any words of wisdom. All I know is that you have a cause. The cause is legitimate, the cause is vital and if we can do a little bit to further the development and the understanding of this disease, then we will have contributed to the world; like Banting (and Best) with insulin.
I’m not telling you that to impress you. That has been the attitude that I have lived with all my life.
Joseph and Rosalie’s grandson Danny Miller is the co-Chair of the JDRF Centre of Excellence Campaign, and Danny’s son Cody has T1D:
JDRF: Mr. Miller, how have your grandparents’ legacy of generosity inspired you?
Danny Miller: Well, how can it not inspire you?
I’ve heard Grandpa say many times that it doesn’t matter whether it’s $2,000 or $2 million; you give what you can if the cause is worthy. And that’s exactly right. What might be a little to me might make a huge difference to somebody else, and that’s always been in the back of my mind. So, I try to live that way, and so do my wife Jennifer and our kids.
It’s really inspiring to see the generosity and the fact that no cause is too small or too unimportant as long as it’s worthy and genuine, then it’s important to support it. That’s what I’ve learned.
JDRF: Mr. Miller, what does the JDRF Centre of Excellence at UBC mean for you?
Danny Miller: Freedom. Being able to relax and not worry about what’s going to happen to my kid at any given time.
Vancouver is already a world-leading research hub for type 1 diabetes research, so the opportunity to take all those world-class researchers and bring them all together and make 1+1 =3 is something that I couldn’t NOT support.
It’s something we had to support because it’s just too obvious, the need. If you take an important cause and bring the best people together and help them work together even better, only good things can happen.
To my grandparents, I’ve said this to you before, thank you so much for taking the lead on this because it’s really important to me and Jen and my parents and Cody and his brothers. It’s just a really important cause and thank you.
JDRF thanks Joseph and Rosalie Segal and their family for their incredible generosity. Their contributions will help to accelerate the most promising research into cures and help us one day realize a world free from type 1 diabetes.
Adolescence can be a challenging time to manage type 1 diabetes (T1D). Life (and hormones!) change in all sorts of ways, and many teenagers experience higher than recommended blood glucose levels as a result, which can mean an increased risk of complications later in life. The study of novel therapies that can improve glycemic control in teens with T1D and reduce the risk of diabetes complications and is critical to improving the lives of youth living with diabetes.
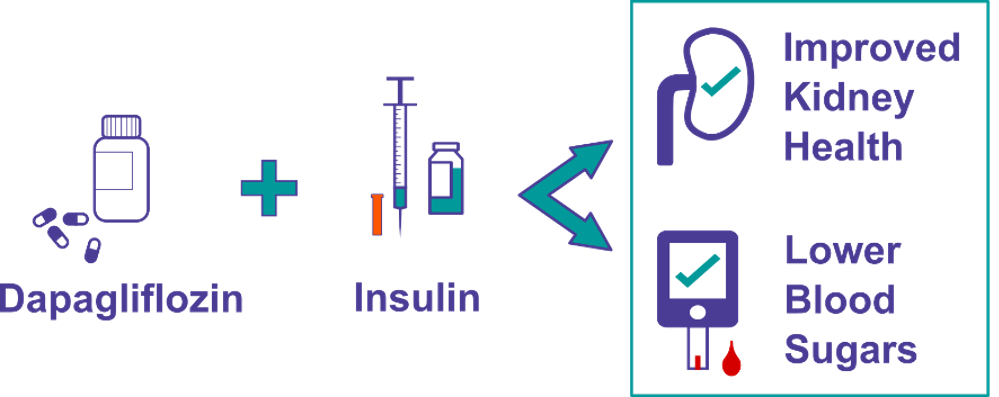
Adjunct-to-insulin therapy – ie, taking another drug alongside usual insulin treatment – is one approach that could help on both fronts. For example, SGLT2 inhibitors are a class of oral medications approved for type 2 diabetes that stop glucose from the blood from being absorbed by the kidneys, instead encouraging glucose to be released in urine. Dr. Farid Mahmud and his team at the Hospital for Sick Children in Toronto are now recruiting for a JDRF-funded clinical trial that will test the safety and efficacy of an SGLT2 inhibitor called dapagliflozin in teens with T1D.
The research team is seeking participants aged 12-18 years with established type 1 diabetes in the Greater Toronto Area (Hospital for Sick Children) and Southwestern Ontario (Children’s Hospital of Western Ontario, London) who may be eligible to participate in the Adolescent Type 1 Diabetes Treatment with SGLT2i for Hyperglycemia & Hyperfiltration trial – also known as ATTEMPT attempt.study@sickkids.ca.
SGLT2 inhibitors such as dapagliflozin can improve blood sugars, increase time in range and decrease kidney pressure, called hyperfiltration. Studies in adults with T1D have shown that SGLT2 inhibitors can lower HbA1c, insulin dose and weight. By alleviating glucose absorption in the kidneys, these drugs can also help prevent long term damage to these organs.
What is the ATTEMPT study?
ATTEMPT is a 22-week clinical trial that aims to determine the safety and effectiveness an SGLT2 inhibitor called dapagliflozin on managing blood glucose and on improving kidney function in adolescents aged 12 to 18 with T1D. The study is being conducted to determine how this therapy can benefit and be used effectively in adolescents with T1D.
ATTEMPT is led by Dr. Farid Mahmud, an endocrinologist and researcher at The Hospital for Sick Children in Toronto. Dr. Mahmud’s overall research focus is diabetes, clinical and translational research relating to other autoimmune conditions (such as celiac disease), and early evaluation and prevention of diabetes-related complications. His research interests include the evaluation of medication and lifestyle interventions in high-risk pediatric groups and the evaluation of impact of the social determinants of health in youth with diabetes. He is also actively engaged in patient-centered research as part of the CIHR Strategies for Patient Oriented Research (SPOR- Can-SOLVE CKD) and as part of the JDRF-funded AdDIT (Adolescent Diabetes Cardio-renal Intervention Trial).
What does joining the ATTEMPT study entail?
Once enrolled in the study, a participant can expect:
5 in-person visits over 22 weeks
A random assignment to the dapagliflozin group, or the placebo group (a small pill that contains no active medicine)
While part of the study, participants will:
Keep taking insulin
Wear a continuous glucose monitor (CGM)
Test for blood ketones
Report any adverse events
Study participants will be compensated and provided support for costs associated with travel or parking. To learn more about the study and how to enroll, please contact: 416-813-7654 ext. 204517 or email attempt.study@sickkids.ca
Canada holds a special place in the story of insulin because scientists Banting and Best made the discovery at the University of Toronto, in 1921. Before the discovery, the lives of people with diabetes were often cut short and the disease often resulted in death. Insulin’s discovery revolutionized the treatment of diabetes, increased life expectancy and changed lives.
One hundred years after the discovery of insulin, Lilly is excited to announce The Leonard Prize, marking the 100th anniversary of the discovery of insulin. To commemorate this milestone, Lilly launched Leonard – a campaign inspired by the life of Leonard Thompson, who became the first person with diabetes to be successfully treated with insulin in 1922, when he was just 14 years old.
Since then, Canadian innovation have come a long way. For example, very recently, Canadian innovation drove the development of the world’s first nasal glucagon for the treatment of severe hypoglycemia. Lilly is proud to recognize the progress made in diabetes and in insulin development over the last century – as well as the advancements yet to come – while also honouring the bravery of Leonard Thompson and the millions of others whose lives were forever changed by insulin.
The Leonard Prize is not just about celebrating past achievements — it’s about recognizing strides made in the development of insulin and other diabetes treatments and using them as inspiration to persevere.
One winner will be chosen from each of five entry categories. A $20,000 (US) grant will be donated in the winner’s name to Life for a Child, an international diabetes initiative that supports children with diabetes in more than 43 countries. The entry categories include:
Teen/young adult: 18- to 25-year-old living with diabetes or with a strong personal connection to someone impacted by diabetes
Advocate/advocacy professional: Active advocate for people with diabetes, either through personal channels or with an established organization
Endocrinologist/primary care physician: Healthcare professional specializing in endocrinology or who acts as a primary care physician to people with diabetes
Diabetes educator/nurse: Diabetes educator and/or nurse specializing in the care of people with diabetes
Researcher: Research professional dedicated to research in the field of diabetes care (therapeutics, technology or otherwise)
Applications can be submitted through an online form when the Leonard Prize site is made available in late June – www.lilly.ca/en-CA/stories/caring/insulin-centennial. Winners will be announced on November 14, 2021 – World Diabetes Day.